Eyes that look more open and refreshed — not simply larger.
"The goal is to take a heavy, sleepy gaze and make it look open and rested. Rather than simply forming a fold, we restore the strength of the eyelid-opening muscle itself."
— Director Choi Dong-Il
A double eyelid procedure that addresses ptosis, opening up a heavy, tired-looking gaze.
When the muscle responsible for opening the upper eyelid is weak, more of the iris is covered than usual — a condition known as ptosis. Ptosis correction addresses this directly, restoring an open, alert appearance to eyes that often look heavy or tired.
Because the procedure requires precise balancing of the eyelid-opening muscles between the two sides, it is technically demanding. We strongly recommend a thorough consultation with an experienced board-certified plastic surgeon before proceeding.
※ Surgical and recovery details may vary depending on the patient's individual condition.
An ideal eye exposes at least 80 percent of the iris when the lids are open.
Distance from pupil center to eyelid margin: 1–2 mm.
Distance from pupil center to eyelid margin: 4–5 mm.
Candidates, technique, and recovery.
Patients concerned with covered iris, persistent forehead lines, or uneven eye sizes.
Non-incisional minimizes scarring; the incisional approach allows for precise scar management.
A more rested expression, with reduced reliance on the forehead muscles to keep the eyes open.
Director Choi Dong-Il personally handles consultation, surgery, and follow-up, drawing on twenty-two years of eyelid surgery practice.
Five clinical situations in which dynamic-fixation ptosis correction is the appropriate choice.
Suspected ptosis
on either or both sides
The iris is significantly
covered when the eyes are open
Forehead muscles or eyebrows
used to compensate when opening the eyes
Uneven eye sizes
between the two sides
A persistently heavy
or tired-looking gaze
When ptosis correction is performed only on appropriate candidates and through the right technique, a brighter, more open gaze can be achieved without significant complications. We do not apply any single approach simply because the patient requests it; the director personally evaluates whether the non-incisional or incisional method is the right choice.
Every diagnosis is performed personally by the director, with sufficient time given to each patient.
Eyelid thickness, levator strength, and skin elasticity are evaluated together to determine the most appropriate technique.
The appropriate technique is selected based on the strength of the eyelid-opening muscle and the thickness of the skin.
An option for patients with thin eyelid skin and reasonably strong levator function.
In the non-incisional approach, Müller's muscle is plicated through the conjunctival surface. This is a reasonable option for slightly small eyes when the eyelid-opening strength is preserved. When levator strength is weak or significant correction is required, the risk of complications increases — for that reason, in our practice, fewer than 20 percent of patients are candidates for the non-incisional approach.
Considered only for patients with thin skin, good levator strength, no significant sagging, and symmetric eyes.
In our practice, the non-incisional approach is performed in roughly 20 percent or fewer of patients, after careful evaluation.


Preserving the orbicularis oculi: a signature technique at our clinic.
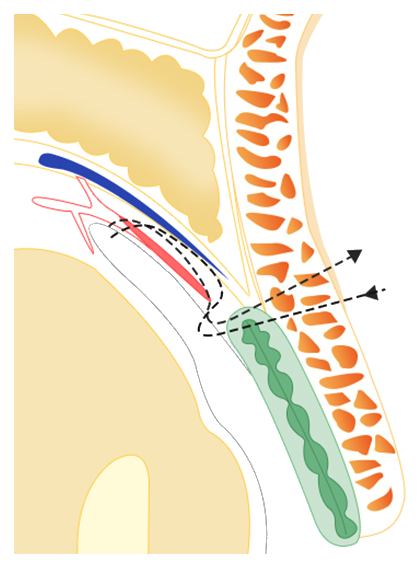
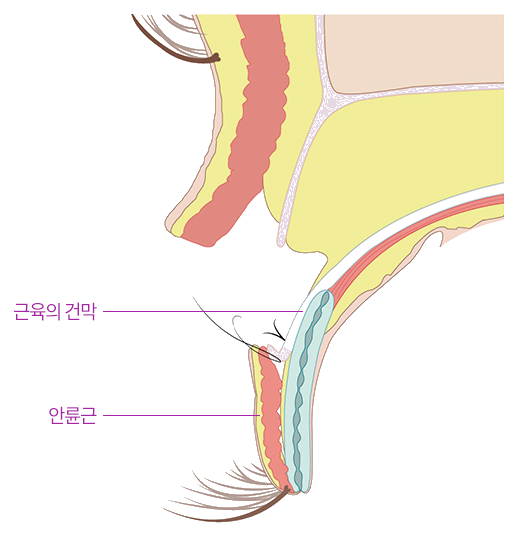
In the incisional approach, the levator aponeurosis is precisely advanced rather than resected. Outside of pathologic ptosis, the muscle itself is preserved; only its terminal portion is advanced and secured by the appropriate amount. Preserving the orbicularis oculi, the muscle responsible for closing the eye, is decisive in determining the result, and is among our signature techniques. The fold is closed with dynamic fixation so that it does not loosen over time.

Unedited surgical and recovery footage, shown for clinical reference.
Unedited postoperative footage, including scar appearance, showing how the dynamic-fixation line settles over time.
Postoperative recovery for a case combined with medial epicanthoplasty, showing how the gaze opens up over time.
Four outcomes patients can expect from dynamic-fixation ptosis correction.
All photographs shown are taken six months after surgery. Additional cases are available in the Before & After section of the menu.








Important considerations before surgery, explained on video by Dr. Choi.
Every inquiry is reviewed personally by Director Choi Dong-Il.