Long time no post.
Today's topic.
Early revision means re-operating soon after a primary double-eyelid surgery — typically when the new crease isn't holding, or multiple folds have developed and the original crease no longer folds cleanly.
The best window is within two weeks of the original surgery, with three weeks as the upper limit. One month is rare and not generally recommended.
This material draws from my September 2021 Eyelid Surgery Study Group symposium talk and a recent case.
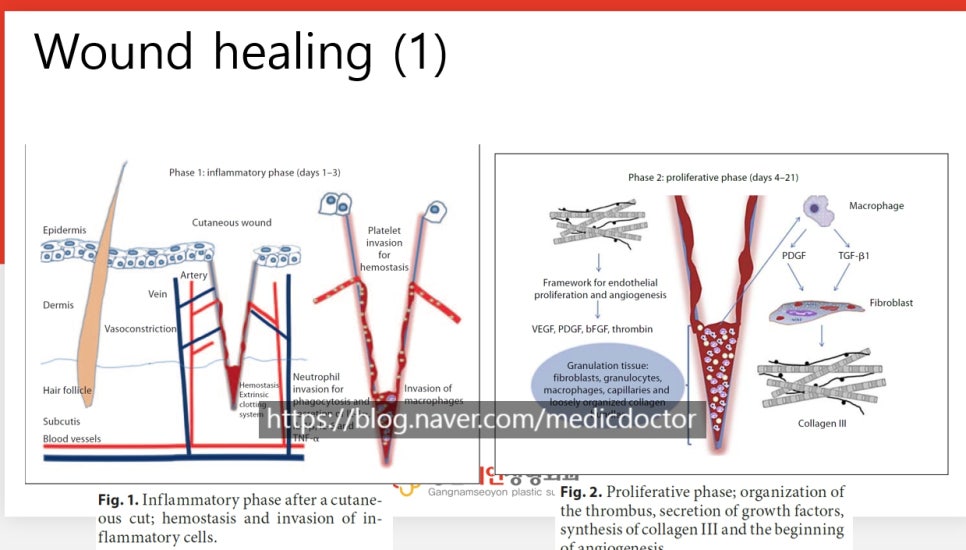
Wound healing begins with the inflammatory phase, where hemostasis takes hold and inflammatory cells move in to clean and start repair.
Here, inflammation refers to the medical sense of the word — the normal cascade of wound healing. This is different from the everyday usage that suggests pus and redness.
Days 4 through 21 are the proliferative phase: clots organize and the wound starts to knit together.
That 21-day mark is the golden window for early revision.
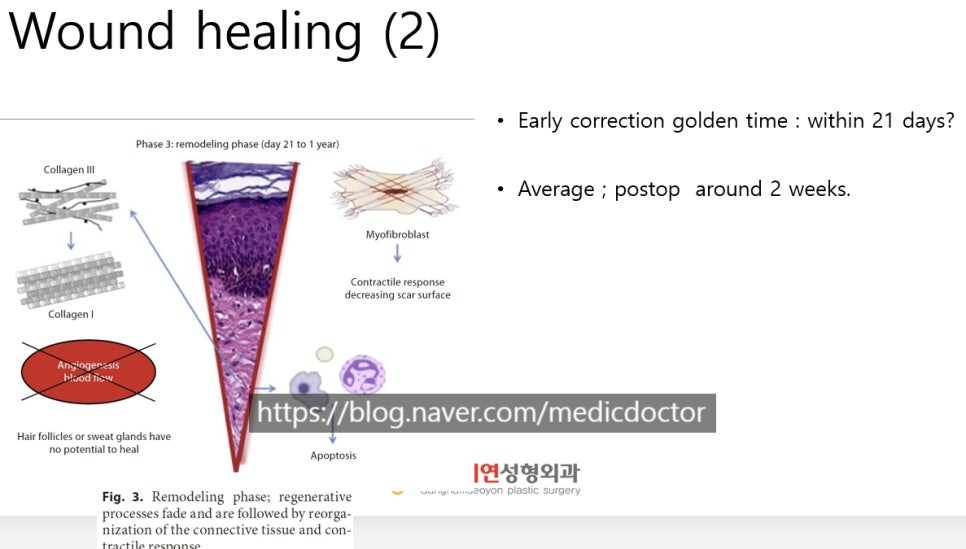
After the third week, the wound enters the remodeling phase. From that point on, the tissue starts to contract and mature, which is what we are trying to stay ahead of.
Up to about one month, we still consider it an early-revision window.
Now to a recent case.
She had been operated on at another clinic two weeks before her visit.
After repeated touch-ups for the crease unraveling and asymmetry, she came to me with multiple folds and difficulty opening her eyes.
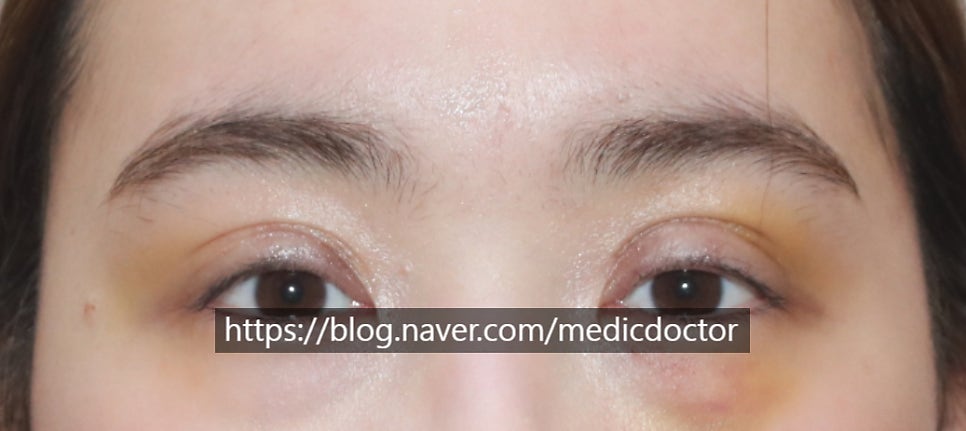
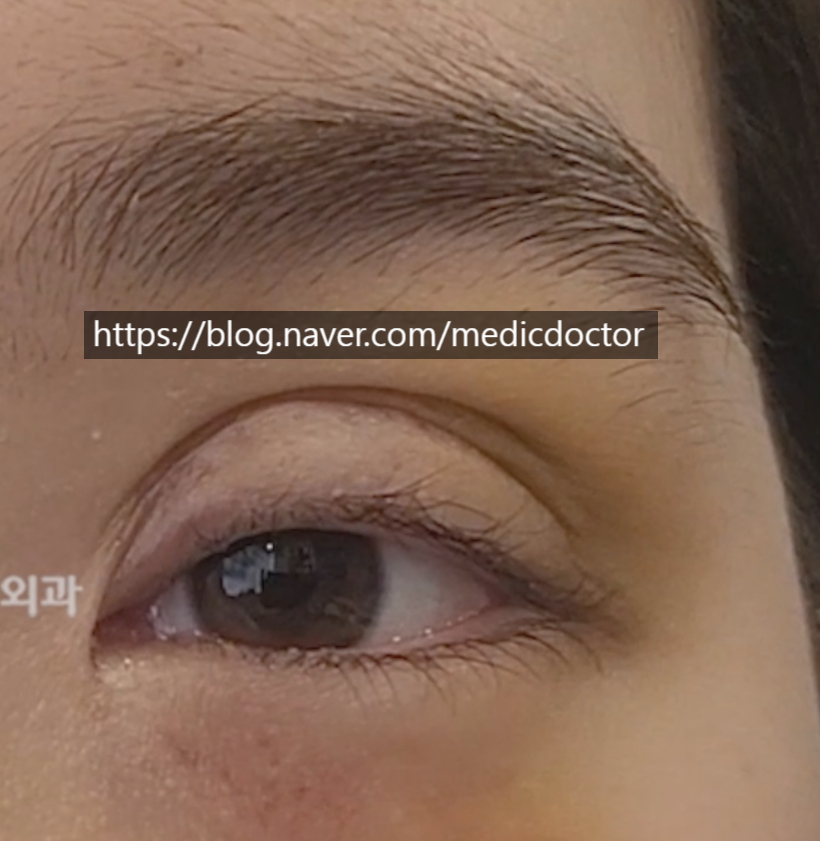
As you can see, both lids show prominent multiple folds and the eyes are barely opening.
Significant adhesions are likely. The good news is that her eyes do open to some degree, which suggests the levator is probably intact.
Patients sometimes worry that multiple folds require fat grafting. In her case, we corrected the problem without any graft.
One week post-op.

No multiple folds, and well corrected.
There is still some swelling at one week.
Looking at her pre-op photo, the medial portion of her left eye (the right side of the photo) is short on skin.
Early revision cannot fix that. It will need to be addressed later, after the skin has had time to relax.
Interim follow-ups will tell us where she is. On video, the multiple folds are gone.
That said, the prior incision on the left side (the right side in the video) sat higher in front, with more skin removed,
which leaves the way the line folds slightly less than ideal.
We may need to revise that at the six-month mark.
My thanks to the patient for placing her trust in us.
Here is roughly how an early revision proceeds.
The ideal outcome is for one operation to fix everything. The reason we do an early revision at all is that operating now is meaningfully better than operating later. We do not do it just because the patient wants it now.
If waiting is the better call, we wait. But because multiple folds rarely improve on their own, we usually intervene early.
Step one: open through the existing incision.
Cutting a new incision and excising more skin makes a clean revision harder later.
Then we open the lid and assess for tissue damage. If there is damage, the priority is repair; aesthetics take a back seat. Treating the function first protects our options at the next revision.
If the eye isn't opening and we wait six months, the levator can retract and scar upward. That loses both function and a clear surgical landmark.
Step two: the shape can be addressed at a later revision.
Prioritizing function can leave a small asymmetry behind.
Some patients tell me, "If we are going to operate twice, why not just wait six months and do it once?" That misses the point.
Once a functional problem is established, it can be impossible to fix later. After losing trust in another clinic, some patients hear me out and still say, "I'll just wait."
It is possible to do the entire repair in one operation later, but I generally recommend early revision: we recover most of the shape and we find out whether there is a functional issue while we still have options.
I'll close with the before-and-after video.