The title sounds heavy, but this case sits close to my surgical philosophy and I wanted to write it up.
First, the term "two-line revision" — patients started using it widely, so I have stuck with it for clarity even though it is not a formal medical term.
Strictly speaking, the technique is a crease-lowering revision that preserves the existing scar. See my earlier post.
I want to share a recent case.

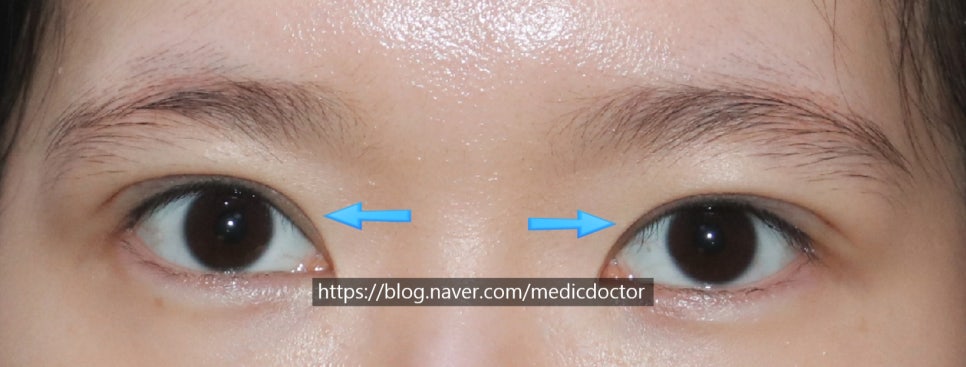
She came in with large eyes and very thin skin, and she felt her crease was set too high.
It really was high. Fortunately her levator function was strong, so the sausage-roll appearance was not extreme — but the crease was very high and the fixation was deep, with a depressed scar.

Her right eye (the left side of the photo) sat slightly higher than the left.

Closed-eye view. The center looks hollowed out, and because tissue is missing in that zone, multiple folds were a real risk after revision.
Many surgeons add a fat graft in this situation. Personally, I am not a fan of fat grafts in this region — I will use one when truly necessary, but I prefer alternatives.
The plan:
1. Begin with a two-line revision, the technique people commonly call "두줄따기."
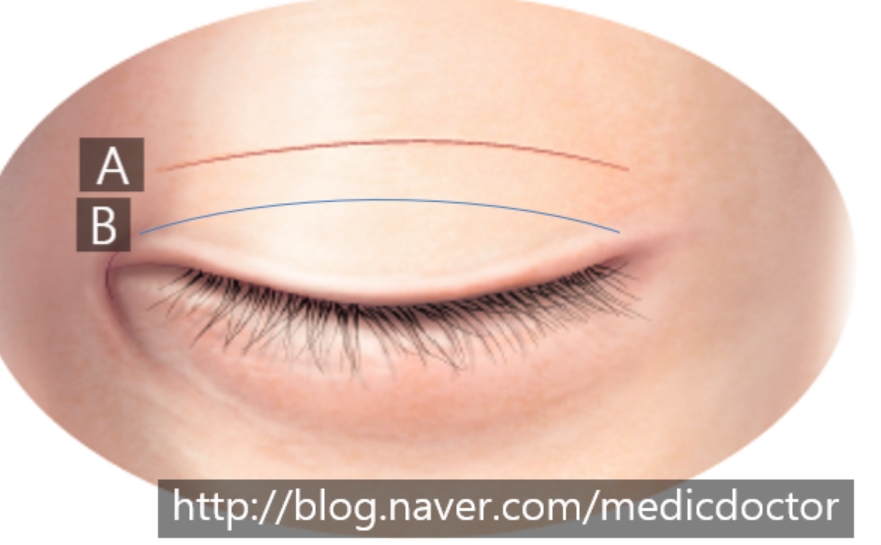
If A is the existing crease and B is the new crease line we design below it, the most cosmetically refined approach is to excise the strip of skin between A and B. Removing it preoperatively makes the operation simpler for the surgeon, but depending on skin quality and other factors a strip that looked redundant on paper can prove insufficient once we are in.
I prefer to err on the side of safety for the patient. So instead of pre-excising the skin, I perform the two-line revision first, and if conditions allow I then trim the old scar to convert it into a single-line revision.
One week post-op.
However, the front of the right crease (her left side) looks slightly low, and the front of her right side looks slightly high.
From the surgeon's standpoint
this is the awkward zone.
I had matched the two sides on the table, but at one week the patient's right looks higher than the left.
In a situation like this I usually wait a week. I let more swelling resolve, and if asymmetry remains, I revise.
I asked the patient to come back at the two-week mark.
The difference was still there, so we trimmed a little more skin from the lateral covered portion of the left crease.

Final view at suture removal.
She is three weeks out from the original surgery, so swelling lingers, but the symmetry is good and she is happy. That makes me happy.
Eyelid surgery is human work, and a small asymmetry is always possible.
Most of the time the difference is from swelling. When the asymmetry is clearly visible, an early adjustment between one and three weeks is usually straightforward.
If I judge that another three months will resolve the difference on its own, I do not perform an early adjustment.
The patient has to trust the surgeon's read on this.
What I tell patients in consultation: "I do not pre-excise the skin. I open, then decide." And: "Trust me on this."
Revisions carry many variables. I can predict about 80 percent of what I will find; the other 20 percent reveals itself only once we are inside.
The more I operate and the more I learn, the more I find myself explaining edge cases to patients. Sometimes I worry I am scaring them.
Our coordinators tell me the same thing. But the great majority of patients leave very happy.
It is just that to cover the rare one-percent complication scenario, I sometimes end up explaining it to everyone, which can leave a patient wondering whether I am even confident in their case.
If I think a case will go well, I recommend the surgery. If I do not, I tell the patient not to operate.
If I am recommending it, that is your green light.