A patient I operated on recently came in for her four-month follow-up, so I am taking the opportunity to walk through her case.
She had previously had an incisional ptosis correction at another clinic and arrived with significant scarring and noticeable mucosal show.
And asymmetry on top of that.

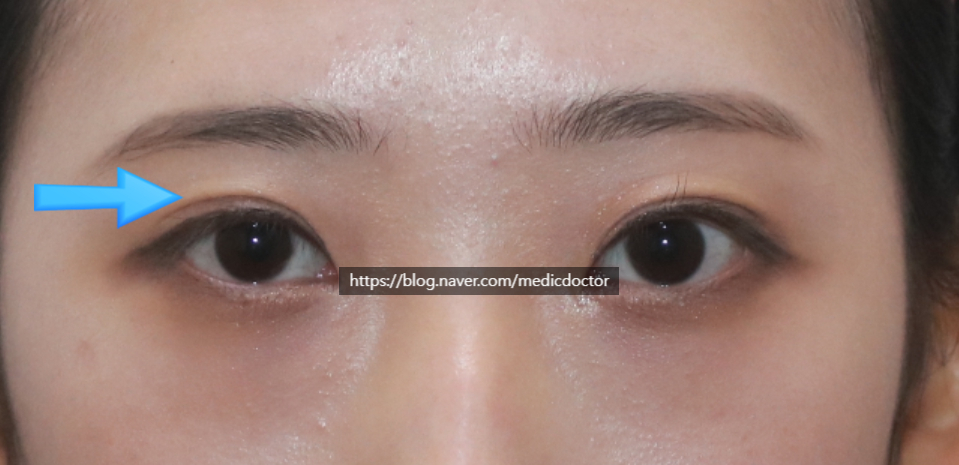
Under low light, the scarring is more obvious.
Look at her left eye (the right side of the photo). After her prior ptosis correction:

There was a depressed scar near the epicanthal fold from forcing the crease into an out-fold, and the multiple folds above it were severe.
On top of mucosal show.

Her opposite eye looks slightly sleepier. In bright light, the levator function on that side is clearly weaker. There is some right-sided facial asymmetry as well, but we can still bring the two sides closer with surgery.
Surgical goals:
Lower the crease.
Address the mucosal show and lash lifting as much as possible.
Convert the out-fold to an in-out fold.
Bring the pupil heights as symmetrical as possible.
Resolve the multiple folds.
We set the new crease low and released the existing adhesions.
For the multiple folds, I personally avoid fat grafting whenever possible, so this patient was managed without any fat graft.
I usually address mucosal show and lash lifting in the same operation, but I never make them the main goal. Setting the fixation gently and at the correct low height usually corrects mucosal show on its own. Going after it aggressively risks functional problems, so I keep it as a secondary objective.
Then I lowered the crease using the double-line technique to convert the out-fold to an in-out fold.
When I opened the right eye (the left side of the photo) intraoperatively, the levator was disinserted and damaged, so we performed a proper ptosis correction. The patient mentioned that she had felt her right eye was congenitally smaller.
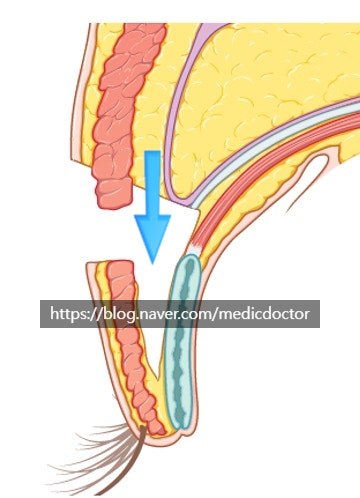
The schematic above is from the Korean Aesthetic Plastic Surgery textbook, Volume 2 (Koonja Publishing).
We dissect the tissue beneath the lid and anchor it lower. The more we dissect, the more the orbicularis oculi (the muscle that closes the eye) can be injured, and that worsens any lagophthalmos.
Four months post-op.
Because of her bony facial asymmetry, her right side still reads slightly smaller, and because we did more ptosis correction on the right, the right eye sits closer to her brow. But this is the closest we can get the two sides to match — most people would not notice the difference.
She placed her trust in us and the surgery went well.
I also released the medial epicanthoplasty scar to keep it from looking depressed.
At consultation I tell every patient that I will do my best — and that I cannot guarantee a result. We always operate to the best of our ability,
but some patients ask the question this way:
"Can you guarantee it'll be corrected? If you can promise, I'll go ahead."
I do not give that guarantee. There are too many variables, and in extreme cases the operated eye cannot be made to look like an unoperated one. Patient satisfaction also varies. That said, when I do recommend surgery, the outcomes are usually good.

Before and after.
Pre-op video.