That is the topic for today.
Over the past decade, ptosis correction has become a far more common add-on to double-eyelid surgery than it used to be.
Many cases turn out beautifully, but the rise in volume has also brought a rise in complications.
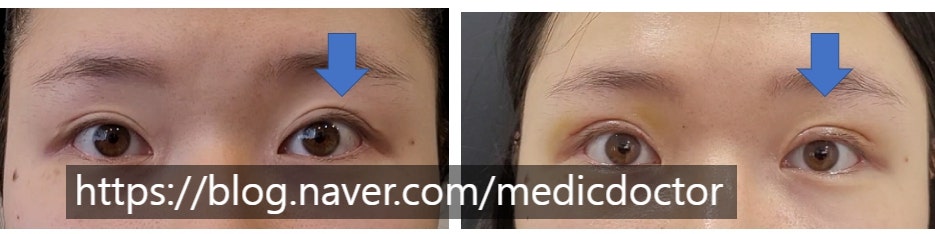
Specifically: a ptosis correction meant to open up small, sleepy-looking eyes is sometimes overdone, leaving the patient with a startled appearance and functional problems.

On opening, the eye does not simply open — it pulls open too far.
First, a quick note on terminology.
Eyelid-retraction repair, as the name suggests, is the surgery to correct retraction.
The term is sometimes used loosely.
Some patients hear retraction and assume it means "setting the levator back" in the sense of weakening it. That is not what the word means.
Retraction means the lid is pulled up too high — exactly the over-opened look in the photo above.
So retraction-repair surgery is the operation that brings a retracted eyelid back down.
At minimum, see a board-certified plastic surgeon who uses the terminology correctly and knows the right technique.
As the photo shows, simply removing the ptosis-correction sutures from the levator does not bring a retracted eyelid back down.
The patient in the first photo had previously gone to another clinic to have her ptosis correction released.
She was told the levator had been released and dissected free of Müller's muscle, but the retraction was not corrected at all.
That alone does not fix it.
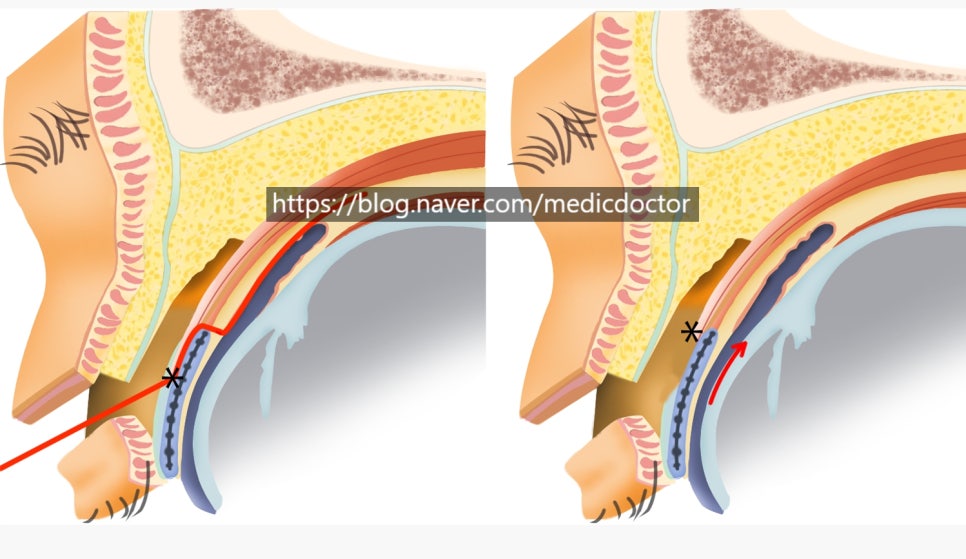
The levator (levator palpebrae superioris) has to be separated from the tarsal plate, Müller's muscle has to be exposed, and Müller's muscle has to be separated from the conjunctiva. That is what a true retraction repair looks like.
That sequence is the heart of the operation. There are several variables along the way, and it is not a procedure for surgeons without significant eyelid experience.

The dissection has to go layer by layer, releasing the adhesions cleanly.
There is significant bleeding, but experienced surgeons control hemostasis well, and the case proceeds smoothly.

With the levator released this way, the retracted eyelid drops back down to the proper level.
This patient at one week post-op. The lateral lifting is well corrected.

Retraction repair carries its own variables.
The eye can look corrected initially and then re-open over time.
If the lid widens again within two to three weeks, an early revision is essential. Compared with other operations, the rate of needing an early revision is relatively higher here. Not every patient needs one — there is no need to worry preemptively.
Asymmetry is also relatively more common than with other procedures. This does not happen in every case either. If the two creases come out different, we plan a re-do at six months. We do not address asymmetry early — there are too many variables in the early period.
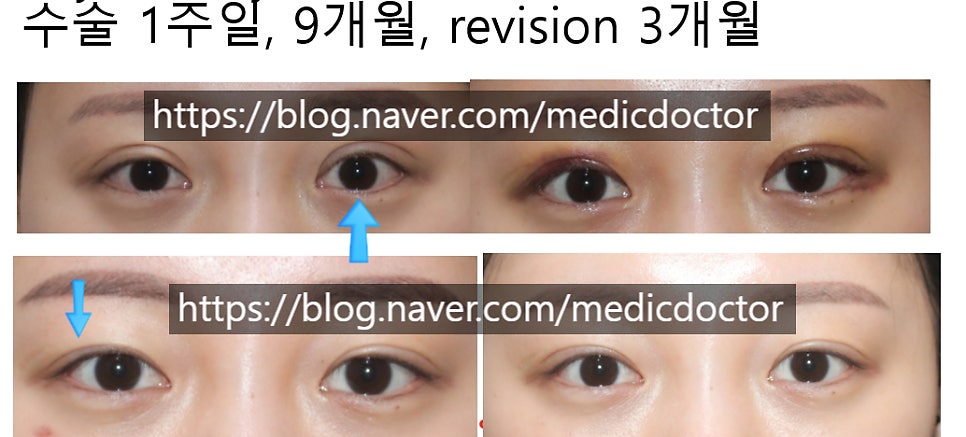
In this patient, the left eye (the right side of the photo) was over-corrected.
We released the adhesions and matched the pupils as closely as possible. The crease on her right eye (the left side of the photo) ended up reading low, so we revised that side.
This is the material I will be presenting at the 15th Eyelid Surgery Study Group Symposium on July 3, 2022.
I hope it will be useful to other plastic surgeons.