I want to walk through the scar-related issues that come up when lowering a double-eyelid crease.
I had this exact conversation with a recent post-op patient, and I am writing it up so there is no unnecessary confusion.
There are several ways to lower a crease — five or six approaches, broadly speaking.
Which one we use depends on the patient's anatomy.
From a scar standpoint, the choice really comes down to two questions.
Do we excise the old scarred skin and lower the crease, or
do we lower the crease while leaving the existing scar in place?
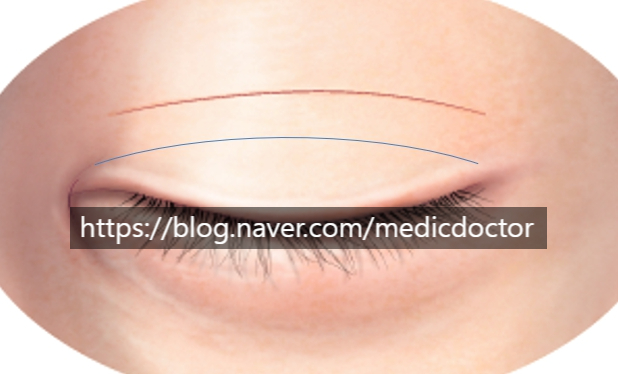
Imagine the upper line is the existing scar and we mark the new crease below it. From here, there are two paths.
We can excise the strip of skin between them and end up with a single scar line, or we can leave it alone and live with two lines.
A single line is cleaner, but it is the wrong choice when there is not enough skin to spare.
When skin is plentiful, this is the best option. The downsides come into play when it isn't:
1. If skin is tight, the conjunctiva can ride up — because the skin is being pulled and anchored from above.
2. In severe cases, lagophthalmos can develop. Scar tissue stretches over time and the lagophthalmos may improve, but as the wound fills in with scar it can pull apart, turning the eyelid scar into a depressed scar or leaving the crease line crinkled.
3. The crease barely lowers at all. For the crease to drop, skin from above the incision needs to fold down and cover it; with everything excised, there is nothing left to drape.
Now the pros and cons of leaving two lines.
Advantages of the two-line approach:
1. The scar tissue is kept in place and used as drape — for a crease to look low, skin above the incision has to fold over the line.
2. When skin is severely deficient, leaving the strip in place reduces tension across the incision and helps keep the wound from spreading.
The disadvantage is the scar.
1. The original scar remains visible. We release the adhesions around it carefully, but the scar itself stays.
And here is the key point: the final appearance of a double-line revision is largely determined by the original scar. The worse the scar going in, the more residual scarring and firmness afterward.
2. If the adhesions are not released thoroughly, multiple folds can develop.
Some patients tell me they have a step-off after surgery.
I should note that the case photos below are cropped from the originals — no Photoshop or post-processing.
All photos are published with the patient's consent.

Pre-op: there is a marked skin shortage at the lateral corners, so the crease does not run all the way out. The skin in those areas is also thick.
She wanted the crease lowered as much as possible. A true hidden crease was clearly not achievable, but I told her I would do everything I could.

Pre-op closed-eye view: from repeated prior surgeries, you can see firm, irregular scarring sitting above the incision line.


One week post-op.
The white tissue above the eyelid scar is the original scar.
Where she is pointing and calling a step-off — as I have explained in earlier posts, when we are trying to prevent multiple folds we temporarily roll a small flap of muscle and tack it; that bulge flattens with time.
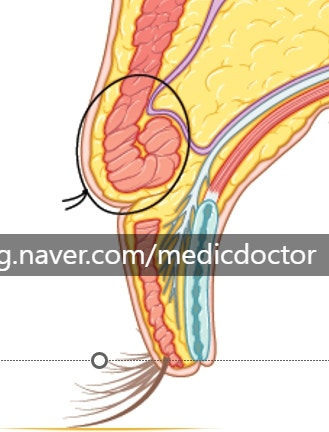
The rolled muscle does flatten, but the upper scar will not disappear. When there is pre-existing scar tissue above it, it really does not disappear.

Four months post-op. The crease has dropped considerably in front. At the lateral end it has come down a little as well, and a crease that previously didn't run all the way out is now visible to the lateral corner.
The thin arrow shows the medial portion, where skin draped down and the crease reads as low. The thick lateral arrow points to where there was a real shortage of skin: the previously-released crease did re-form, but it is more visible than the medial portion.

Scar at four months. The fullness she had been calling a step-off has resolved, but the firm ridging from the original scar is still there.
There was an unexpected wrinkle near the medial canthus on the lateral side. As the scar matured, a small amount of skin laxity appeared in front, and that laxity ended up draping over the crease more than at the lateral corner.
Laterally, where skin was very tight, the scar reads flatter but the crease is more visible. Medially, the thick pre-existing scar tissue ended up covering the crease.
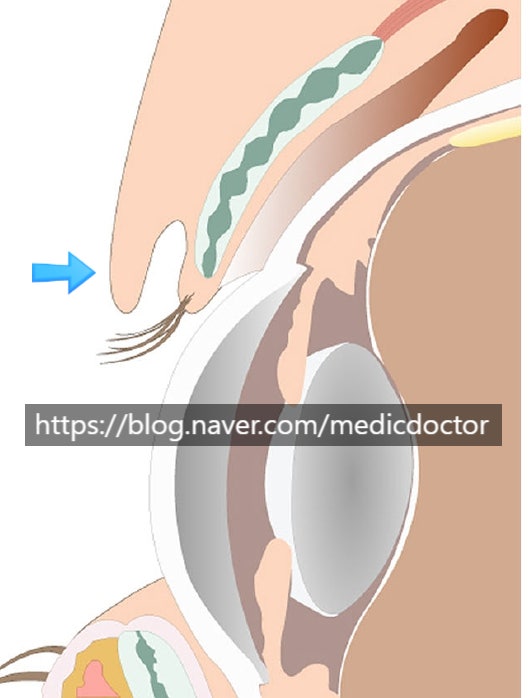
The arrow marks how much residual scar tissue is sitting on top of the crease.
You may be wondering how this can be addressed.
1. If the lateral crease drops a little further as remaining swelling resolves, the whole lid may settle into a soft hidden-crease look. Her skin is on the thicker side, so I had expected the crease to remain faintly visible rather than disappear; the medial portion is more covered than I anticipated, which suggests the lateral side may not drop as much as we hoped.
2. The most realistic fix is to either excise a small amount of skin medially or raise the line back up in front. Raising the medial portion alone, while leaving the lateral untouched, would not balance: the original lateral crease was higher than the medial one to begin with, and the line was simply released at the corner so it didn't read as obviously high.
The cleanest plan is to trim the protruding scar slightly in front so the medial crease reads as a low fold, which makes the entire lid look like a low double fold. The end-state would be roughly what we saw at one week post-op above.
If a touch-up is needed, I will do my best to refine it.
Cosmetic surgery is human work, and revisions in particular sometimes need a second-stage refinement. We do that as needed.
Before any double-line revision, I make a point of telling patients clearly that the scar will not disappear. The other case photos here all show the same thing.




At one week post-op, you can see the temporary fullness patients sometimes call a step-off. That bulge resolves, but the white scar tissue itself does not.


One month post-op — still present, and typically starts to soften from around three months.


Three years post-op. The patient came in for a long-term follow-up and you can see the white scar above the incision marked by the arrow. It is still there, but the step-off is gone; only a thin line of scar tissue remains slightly raised.
Will revision surgery erase the scar?
I understand wanting to improve a poor first result, but any incision creates a scar. The original scar will not disappear unless it is excised.
And depressed scars are softened by recruiting surrounding tissue over them — they cannot be erased.
We will continue to give every patient our best work at Gangnam Seoyon.