The title is a mouthful. I had this conversation with a patient at a recent follow-up, promised her I would write it up, and here it is.
When we lower a crease using the double-line technique, the new crease often ends up significantly lower than the original.
Up front: at Gangnam Seoyon, we do not use deep fixation.
For the technique itself, please see the earlier post.
When patients ask for the crease lowered as much as possible, sometimes they want the fold to be nearly invisible.
Men in particular often want this; some women do too.
Here is a double-line revision example, in a patient who wanted a hidden-crease look.

One week post-op. You can see a slight fullness sitting just above the incision.
When patients see this small bulge, the most common misconception is to assume the suture was tied down too deep.
It isn't.
Then what is it?
There are two reasons.
1. Surgical technique. The double-line approach is prone to producing multiple folds. To prevent that — especially when the surgeon is less experienced — we build in a small safeguard.
That safeguard prevents multiple folds. If you have followed me for a while, you know I rarely tape the eyelid post-op. I only do so in the rare case of very thin skin or specific situations.
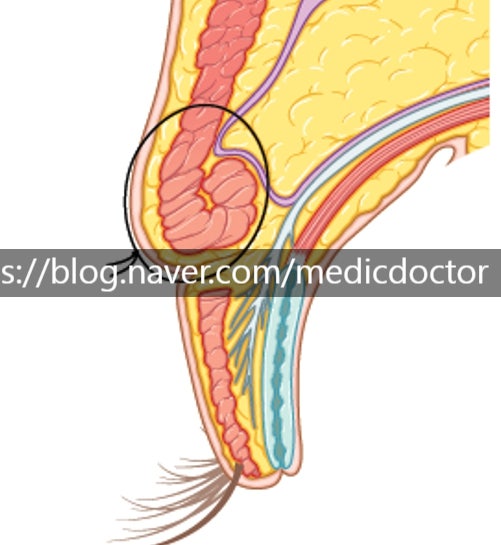
2. When the crease has been set low and skin is in short supply, the fold has to show somewhere. We deliberately leave skin above the incision so that it can drape down over the crease and keep it concealed.
What does that mean.
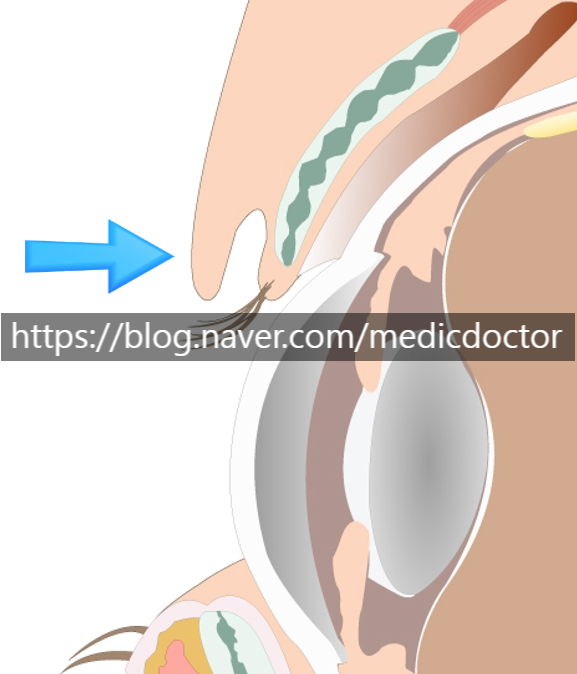
We leave the strip of skin marked by the arrow sitting above the eyelid crease incision. The illustration is from "Ptosis Correction in the Monolid," which I published in 2018 in Aesthetic Plastic Surgery — the first article on the technique to appear in the U.S. aesthetic literature.
Watch this video.

When the eye is closed, the small fold you see is not a scar. It is the strip of skin we left above the incision, designed to drape over the crease when the eye opens.
If a patient really doesn't like the look, we can excise that drape — but the crease will then be visible, and the line will not sit as low as they wanted. Raising the crease is generally the better option than excising the drape.

When the skin is stretched flat, the fold reads as a faint line. The white you see is sunscreen settling into the fold.
I hope that clears up the misconception about deep fixation.
When a plastic surgeon talks about deep fixation, this is not what we mean.

Deep fixation looks like this — a tethered, depressed scar.

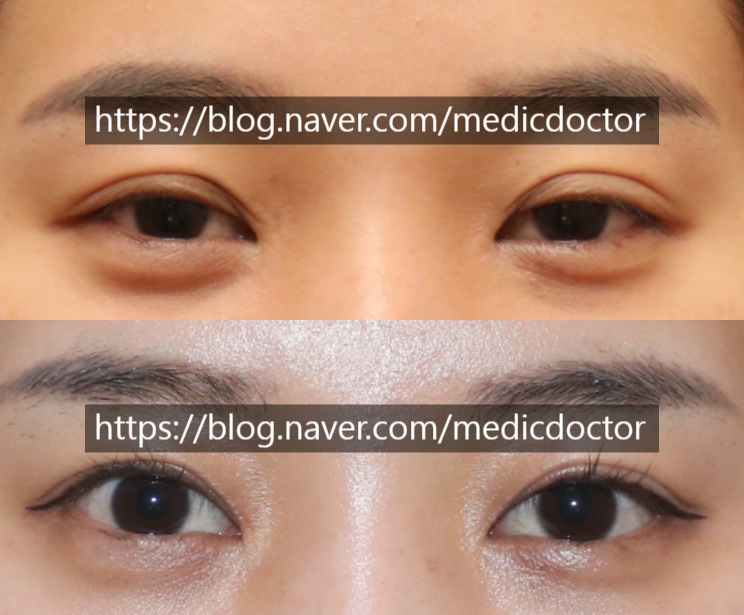
On the left, the trapped, pinched-looking lid; on the right, the same lid after a double-line revision lowered the crease and improved the scar. The upper arrow points to the original scar; the lower arrow, to the previous fold.
We use shallow fixation to minimize scarring.
The folded look I described above continues to flatten with more time.
From our textbook (Aesthetic Plastic Surgery, Koonja Publishing): a depressed scar generally flattens over time. But when the crease is lowered substantially, as I described above, skin will end up draping over the incision. The more prominent the eye, the flatter the lid reads; the more deep-set the eye, the more skin folds down over the crease.
Without that context, junior surgeons and patients alike are well-positioned to misread the early result.
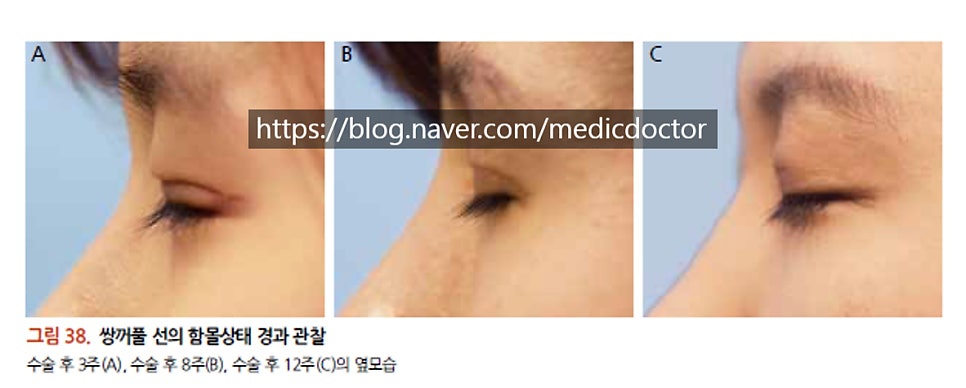
For reference, even ordinary incisional scars can look uneven and ridged in the early period.
They typically firm up through three months and start to soften from six.
Judging a scar at one month is simply too early.

Even if the scar marked by the arrow looks kinked, it settles into a clean line on its own.
Revision patients often come in asking us to fix their scars.
Scars can be improved, but not erased. A severe scar that has already formed will soften, but it will never disappear — and patients who come in asking us to remove it should know that going in. When the eye is open, our priority is a beautiful result; for the scar, we promise to do our best. Any incision creates a scar. We do everything we can to make it inconspicuous, as in this patient. But asking for an invisible scar is asking too much. Healing biology varies between patients, and we have no way of knowing exactly what is going on inside the lid before we open it. We do not guarantee a 100% scar-free result. We promise our best effort.


Pre-op, three years post-op closed-eye, three years post-op open-eye.