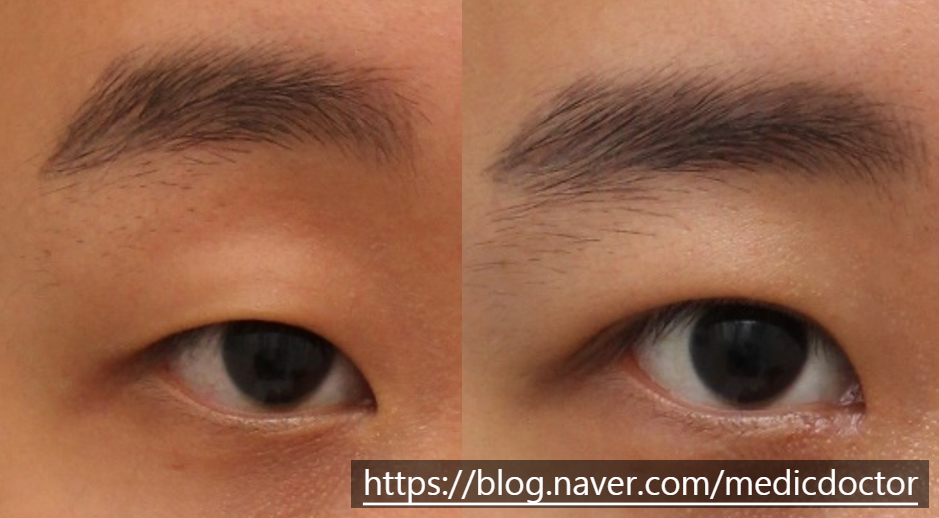
Most male patients I operate on receive an incisional ptosis correction; only a minority are good candidates for the non-incisional version.
Men in whom the non-incisional approach is not advisable. Check whether you fit any of the categories below.
1. Thick skin.
Male skin is reliably thicker than female skin, which means buried sutures release more easily.
From the surgeon's standpoint, longevity matters — and we choose the technique that holds.
2. Weak levator function.
Patients with markedly sleepy eyes get little benefit from a non-incisional approach.
Forcing aggressive tightening in this setting produces a strong pulling sensation and fails to deliver a real correction.
Severe pulling sensation can disrupt sleep.

3. Revisional cases.
Revisional cases must be done incisionally.
Done non-incisionally, you can end up with multiple folds, no real correction, and wasted time and money.
4. Excess fat.
If fat removal is needed, a buried-suture (non-incisional) approach is unsuitable.

5. Pre-existing natural double-eyelid crease.
If the existing crease is not first released, you cannot set a low crease and have the upper skin tuck inward to hide it. Instead of one fold, you end up with multiple folds.
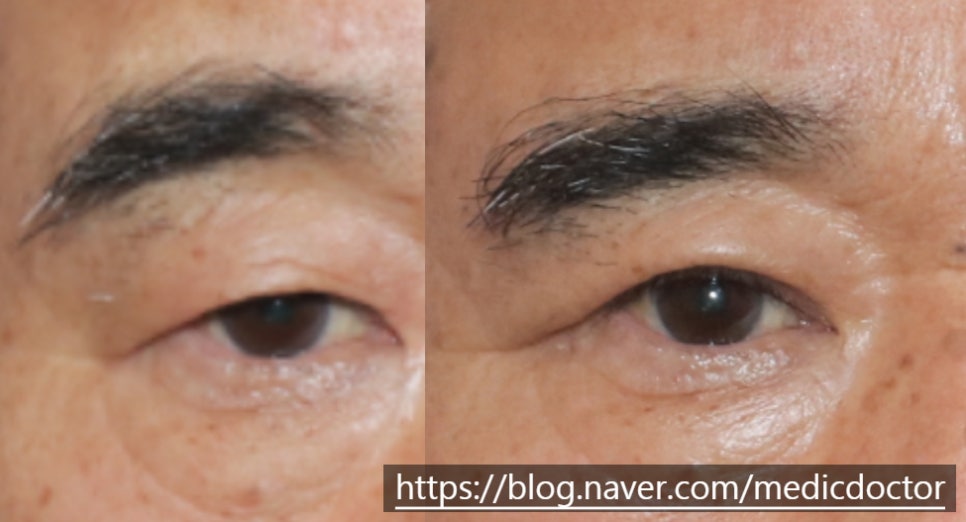
6. Eyelid skin laxity (especially in older patients).
So who is a good candidate for non-incisional ptosis correction?
1. Patients with thin skin.
2. Patients with strong levator function and minimal skin sagging.
This material is based on a paper I presented at the American Society of Plastic Surgeons in 2018 — the first international report on this approach.
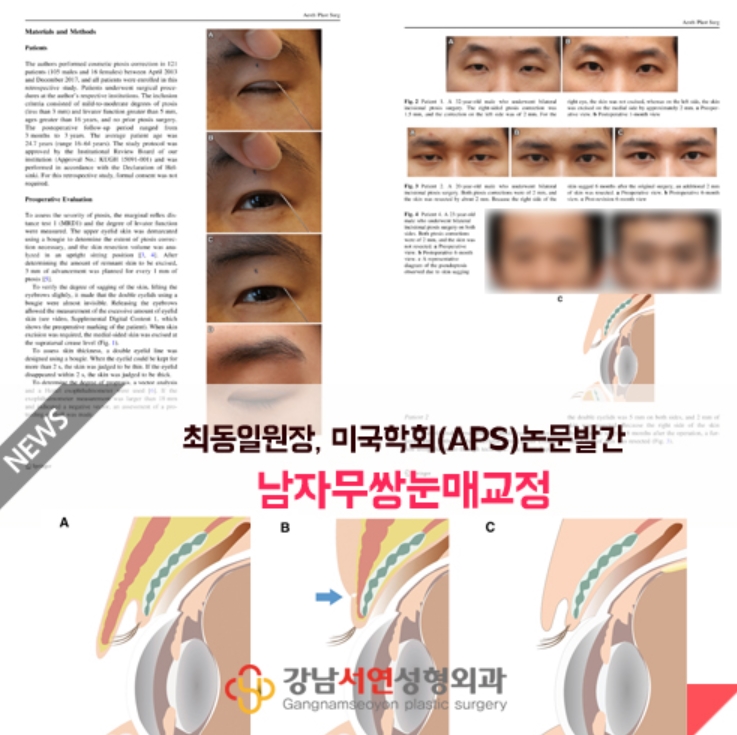
Built on lectures I gave at the 2019 fall continuing-education course and other meetings.