It's been a while since my last post.
A note on severely asymmetric eyes.

On one eye, the crease sits heavy and the conjunctival mucosa is visibly pulled up.
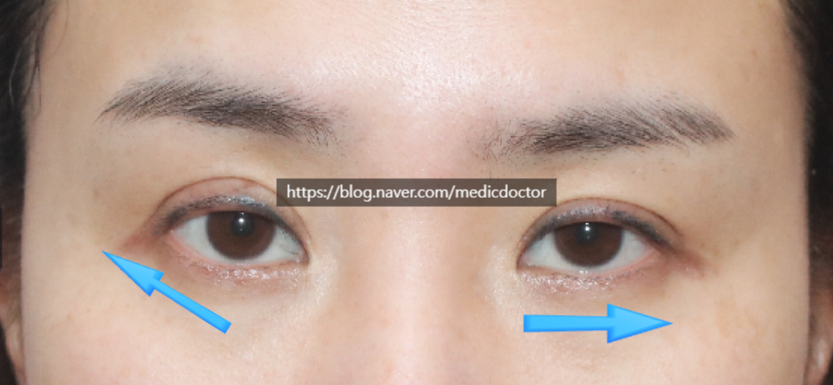
Comparing both sides, the asymmetry is striking.
There's underlying facial asymmetry as well, which makes the right outer canthus sit higher.
The outer canthal angle takes on an arrow-like shape.
The crease itself is an outer-fold pattern, sitting noticeably high.
Anatomically, the crease isn't actually placed high — the limited amount of remaining skin is what makes it appear that way.
The same skin shortage pulls the lid upward, exposing the mucosa.
In the pre-op video, the scarring is significant, the skin is severely lacking, and the mucosa is pulled up.
Why does the mucosa lift like this?
See the earlier post for the full explanation.
Mucosal Show, Lash Lift, and Upper-Lid Ectropion After Double Eyelid Surgery
I've covered this in earlier posts as well.
When skin is severely lacking, pushing too hard to fix the mucosal show can lead to functional complications.
We discuss this thoroughly with every patient before surgery: in severely compromised cases, some degree of residual mucosal show will inevitably remain.
Substantial improvement is still possible.

One week post-op. The eye won't return to a never-operated appearance, but the improvement over the pre-op state is clear.
Substantial post-op improvement, in my view.
Looking at the pre-op view, the patient's right eye (left on photo) had a high outer canthus and a high crease, which gave the eye a triangular shape.
Understanding the baseline matters above all, because the underlying bony anatomy cannot be changed. Patients should hear a complete explanation, understand what the procedure cannot achieve, and proceed with realistic expectations.
Severely compromised eyes generally cannot be made to look unoperated. Meaningful improvement is the realistic goal.
I'll continue to do my best for every patient.