I have been seeing more patients lately who come in already worried.
Especially those who have spent time on Korean YouTube, online cafes, and the like.
Some arrive convinced that ptosis correction always produces complications.
Is that actually true?
No. Ptosis correction is an excellent operation when properly indicated. So why do complications happen?

Because the wrong procedure was chosen for the patient — or, occasionally, because the patient is unusually sensitive.
What follows is my own experience and opinion. Other surgeons may disagree.
First: poorly chosen technique.
1. The wrong surgical method.
Take buried-suture (non-incisional) ptosis correction. In my hands, it is reasonable only for very mild ptosis — patients who open their eyes nearly normally and want a slightly larger eye.
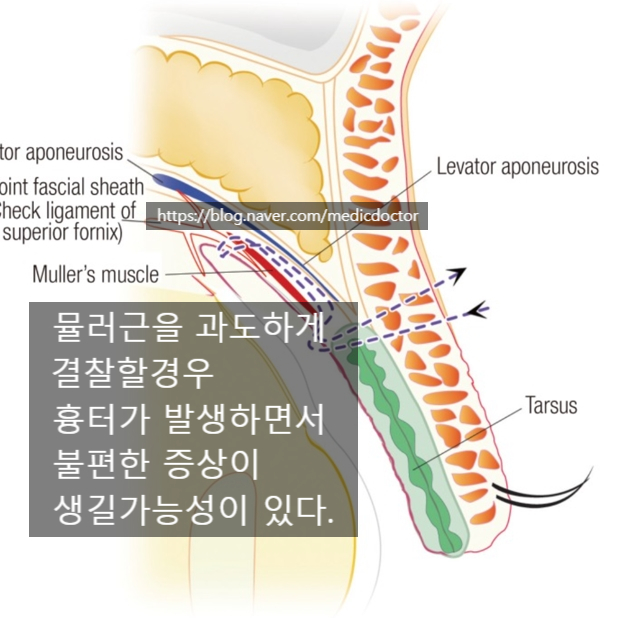
When a surgeon over-tightens Müller's muscle (part of the eye-opening apparatus) through a transconjunctival approach, the patient develops a strong pulling sensation.
In those cases, an incisional approach using the levator aponeurosis is far more comfortable for the patient.
2. Moderate to severe ptosis.
These patients have a weakened, less elastic levator to begin with.
It is a congenital weakness. Imagine the biceps in an underdeveloped arm: even repeated effort cannot fully strengthen the underlying muscle.
You can mechanically force the arm into flexion, but extension becomes harder. The same logic applies here.
When we shorten the levator aggressively in such cases, the eye does not close fully. Humans adapt — closure improves over time, and most patients do well, often only sleeping with a slight gap. Major complications are uncommon.



3. Complications specific to incisional ptosis correction
and how they arise.
These are really problems of incisional double-eyelid surgery rather than ptosis correction itself. Incisional surgery is now usually combined with ptosis correction, and an inexperienced surgeon or non-specialist who handles the orbicularis oculi too aggressively can damage it.

Damage to the orbicularis below the crease line leaves the eye unable to close.

That can result in permanent incomplete closure, severe scarring, and various other complications.
Then there is the sensitive patient.
Some patients get headaches from a new eyeglass prescription, or pounding heads from coffee.
Honestly, when a sensitive patient develops complaints, there is no easy answer. It can happen with incisional ptosis correction, with simple incisional double eyelid, even with a buried-suture procedure.
Even a basic buried-suture double eyelid can cause issues. For someone with that kind of sensitivity, I usually recommend not having surgery at all.
When the surgery is performed well, more than 99 percent of patients do fine. Medicine never offers 100 percent, so I leave the one-percent margin honest.
Avoid over-manipulation, avoid repeated re-operations, and especially with a first surgery the odds are very good. See an experienced board-certified plastic surgeon and proceed with confidence.
An older newspaper interview, attached for reference.