
Some patients have congenitally heavy, sleepy-looking lids that simply don't open well.
In these cases, conventional ptosis correction often fails to enlarge the aperture.
Standard ptosis correction will fall short here.
Effective correction requires identifying and working on a deeper structure called the conjoint fascia sheath (CFS).
The procedure is technically demanding and is generally performed by experienced plastic surgeons.
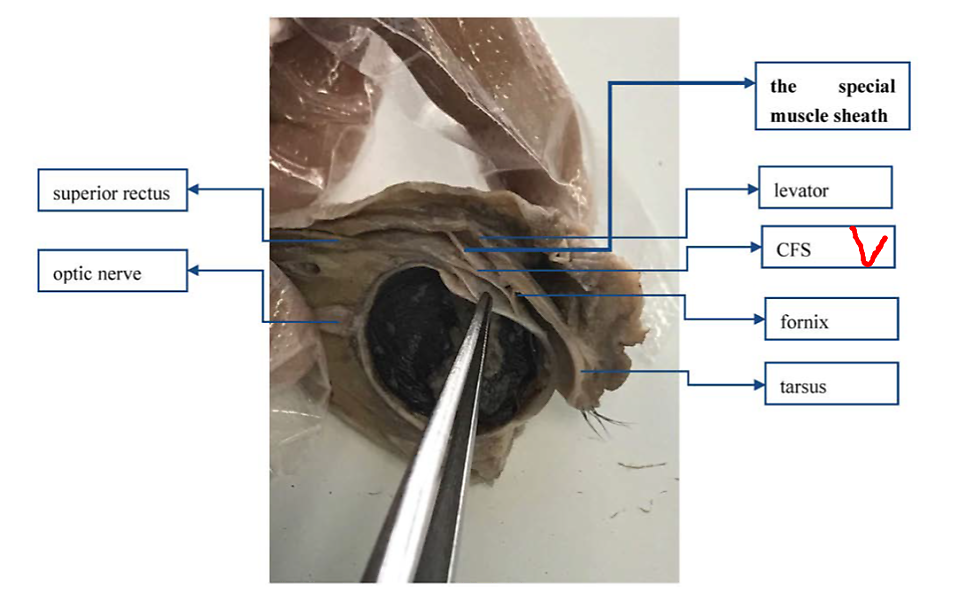
The structure marked above is the CFS, which sits closely along the top of the globe.
It's difficult to locate, difficult to dissect, and a structure most surgeons hesitate to operate on without considerable training.
The procedure was first introduced by Holstrom; Korean surgeons have refined and developed it substantially, and Chinese surgeons have since adopted the technique widely.
This patient came to us in this condition after surgery elsewhere. She had congenital ptosis on one side; the prior surgery had not opened the eye, and now the lid neither fully opened nor fully closed.
Immediate post-op view. The eye is opening well, though it does not fully close yet.
This will improve with time.
Two years post-op. The iris exposure is now nearly symmetric, and the lid closes well.
Achieving perfect symmetry is difficult when one side has severe ptosis, but a close match is realistic.


Before-and-after comparison.
I'm pleased with how it turned out.